On April 8th, 2024, a total solar eclipse will sweep across North America, from Mexico to the Maine-Canadian border. For those who experienced the spectacular solar eclipse of 2017, this one will be similar, crossing the United States from west to east and passing...
Most people find being inside a hospital a bit uncomfortable, as a patient or otherwise. But I find hospitals familiar and comforting, which isn’t surprising considering how most of my early childhood was spent in one. When I was three years old, I was diagnosed with Acute Lymphoblastic Leukemia, or ALL. My bone marrow had started to produce immature mutant versions of healthy white blood cells, crowding out my working immune system. Leaving me open to infections and so weak I couldn’t walk. Back then the standard treatment for pediatric ALL was high dose chemotherapy. These drugs killed off the cancerous cells by preventing them from dividing, but they also had the same effect on healthy cells, weakening and stressing my body even further. It took months of intensive chemo and years of recovery, but my ALL eventually went into remission. I don’t have many memories of the time, but my family and those with loved ones who have dealt with cancer know how much of a battle chemotherapy is.
Unfortunately, even a quarter of a century later, treatments for ALL haven’t fundamentally changed. But in the last decade biomedical scientists have begun developing a new generation of treatments called immunotherapy that don’t use harsh chemotherapy or radiation, but instead compel the patient’s own immune system to fight cancer as it would fight any common infection.
Several therapeutic strategies fall under the category of immunotherapy. Some have been utilized for years, while others are so cutting edge they have only become possible through the newest research on how cancer and our immune systems interact.
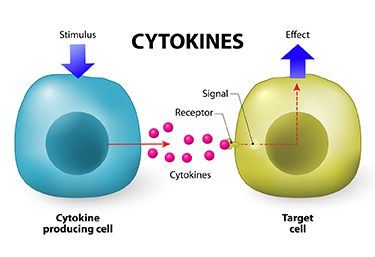
Cytokine Therapy
The immune system is made up of dozens of different types of cells which all communicate with each other and other tissues using chemical signals called cytokines. When the body detects signs of damage or infiltration by foreign bacteria, cytokines are released at that site to draw in T-Cells, neutrophils, macrophages and other immune cells to deal with the threat. This local immune response is called inflammation. We see it in the swelling around infections or wounds caused by blood vessels dilating and becoming leaky to allow fluid and immune cells to flood into the area.
But very often cancer doesn’t cause high levels of inflammation. The body may mount an inflammatory response, but not enough to damage the tumor. Or the tumor may secrete its own cytokines which dampen inflammation itself.
Instead, by administering the right artificially synthesized cytokines through injections, doctors can stimulate the immune system to redouble its response. Newly alerted, immune cells can infiltrate and begin to slowly shrink a tumor.
Checkpoint Inhibitors
T-cells are the hunter-killer cells of the immune system. An army of patrolling T-cells constantly inspect cells to differentiate what is foreign to the body from what belongs. Once they find an abnormal cell they initiate an all-out immunological assault. But checkpoint pathways are in place to make sure these assaults don’t progress too far. For instance, on their surface, T-Cells have the aptly named Programed Death receptor, PD-1. When the ligand, or activator, of PD-1 binds to the receptor it trips the T-cell’s kill switch and cuts off the T-cell response.
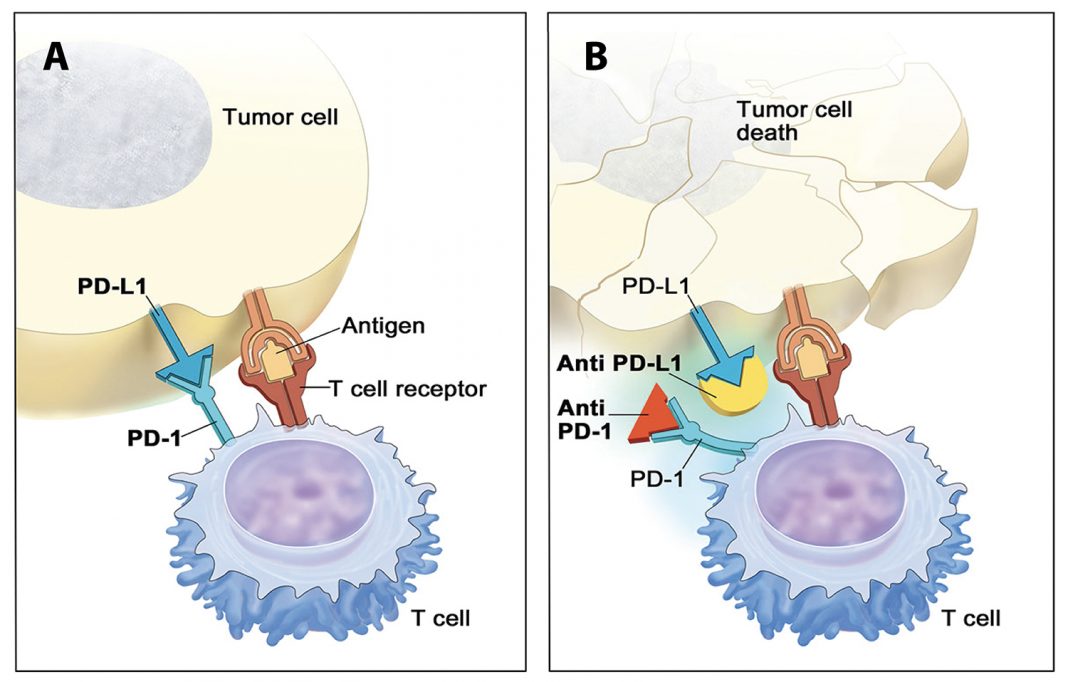
Some cancer cells hide from T-cells by expressing PD-1 ligand on their surface, thereby stopping T-cells from accumulating and recognizing their cancerous nature. New drugs designed to block PD-1 or its receptor from activating the kill switch permit T-cells around a tumor to survive and recruit more T-cells to dissolve the tumors.
CAR-T Therapy
The newest, and perhaps most powerful, immunotherapy is the Chimeric antigen receptor T-cell, or CAR-T, therapy, which uses a patient’s own reprogrammed T-cells as ‘living drugs’ to attack cancer.
Immune cells use receptors to recognize threats like bacteria and viruses by their antigens, the foreign proteins and molecules on their surfaces. But because cancer cells are your own cells, their antigens don’t register as alien. Fortunately, certain types of cancer display antigens that aren’t present on the cell-types they mutated from, making them unique to the cancer. So, while the body may not naturally target those antigens, scientists can engineer artificial antibody-like receptors called Chimeric Antigen Receptors, or CARs, that could allow T-cells to differentiate cancerous cells from healthy cells.
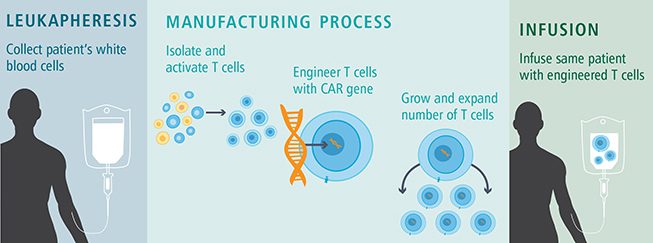
Creating CAR-T cells is a complex process. The first step involves filtering the patient’s blood to isolate a few thousand T-cells. These cells are then sent to a lab where an artificial gene is inserted into the T-cells genome. This gene encodes the blueprints to build the specifically designed CAR tailored to an antigen on the patient’s tumor cells. The T-cells that start expressing the CAR on their surface are then grown in an incubator until a few hundred cells become millions. While these cells are multiplying, the patient receives a low dose of chemotherapy. The purpose isn’t to kill the tumor but to remove enough of the patient’s normal T-cells to allow room for the CAR-T cells to take hold. Finally, a single dose of freshly grown CAR-T cells are infused into the patient. Once the engineered T-cells engraft, they start to recognize the tumor’s antigens through their CARs and begin secreting cytokines to mobilize the immune system to eat away at the tumor. Instead of the terrible side effects of chemical chemotherapy or radiation, many recipients of CAR-T therapy feel as if they are fighting a bad flu, all while their condition improves.
The number of clinical trials for CAR-T therapies has been exploding in recent years. And many more are just beginning. CAR-T therapy has already been used successfully against certain B-cell cancers that didn’t respond to traditional treatments. In these cases the CARs targeted an antigen called CD19. These CAR-T cells also targeted a patient’s healthy non-cancerous B-cells, but if given the right care, those non-cancerous B-cells are naturally replaced by the body once the cancer is gone.
Refining Immunotherapy
Even with their successes, many immunotherapies are so new there isn’t yet enough clinical data for scientists to fully understand the range of side effects and exactly how to optimize treatments. Immunotherapies carry the risk of a devastating side effect called a “cytokine storm”. This occurs when a flood of cytokine signals hyperactivates the inflammatory reaction, leading to severe fever, fluid buildup in the lungs, and even death if not treated quickly. Some reports have also linked neurological side effects to immunotherapy, but studies are ongoing.
CAR-T therapy too, while the most promising, is expensive and time consuming using current methods. It takes weeks to isolate, engineer and grow the modified T-cells, and every step needs precise measures to ensure that a single dose will perform exactly as expected. These limits hinder immunotherapy’s potential, for now.
While the chemotherapy protocol I underwent hasn’t changed in two and half decades, it has been greatly refined, becoming safer and precise. So we can expect these and other immunotherapy strategies to grow and develop in the next few decades. But, for all its promise, immunotherapy probably won’t end up a universal treatment against cancer. Nevertheless, it represents another option in a doctor’s arsenal to treat disease and prolong life.