On April 8th, 2024, a total solar eclipse will sweep across North America, from Mexico to the Maine-Canadian border. For those who experienced the spectacular solar eclipse of 2017, this one will be similar, crossing the United States from west to east and passing...
If you’ve been diagnosed with a rare disease or a condition your doctor is unfamiliar with, the idea that scientists are working night and day to help you isn’t always a comfort when you’re lying in a hospital bed. Biomedical research takes a lot of time and money, all the while thousands of patients and their families sit and hope. The unprecedented and rapidly evolving COVID-19 crisis has stressed this country’s medical system nearly to its breaking point, but medicine has reached the point where nothing is truly unfamiliar. Coronaviruses have been studied for decades, and how respiratory viruses damage our lungs is a field of study unto itself. It’s only a matter of applying the tools we already have to develop new treatments and vaccines to combat this new virus.
When the news and scientists talk about COVID-19, they are referring to the medical condition, while the virus which causes COVID-19 is called severe acute respiratory syndrome coronavirus 2, or SARS-CoV-2. For most, the symptoms of SARS-CoV-2 infection include fever, cough, shortness of breath, and fatigue, and can last for weeks or more. But, unfortunately, for a few COVID-19 patients these symptoms get worse and can become life-threatening. This exacerbation very often leads to what doctors describe as acute respiratory distress syndrome, or ARDS. Many unrelated diseases and conditions can lead to ARDS, not just respiratory viruses like SARS-CoV-2. ARDS occurs when the immune system disrupts the lung’s normal functioning, and despite years of experience with ARDS doctors have no true cure, only treatments to lessen the severity. The mechanics of how we breathe and how ARDS affects the lungs are already understood, but COVID-19 is forcing doctors to reconsider old practices in the pursuit of new treatments.
How the Lungs Breathe
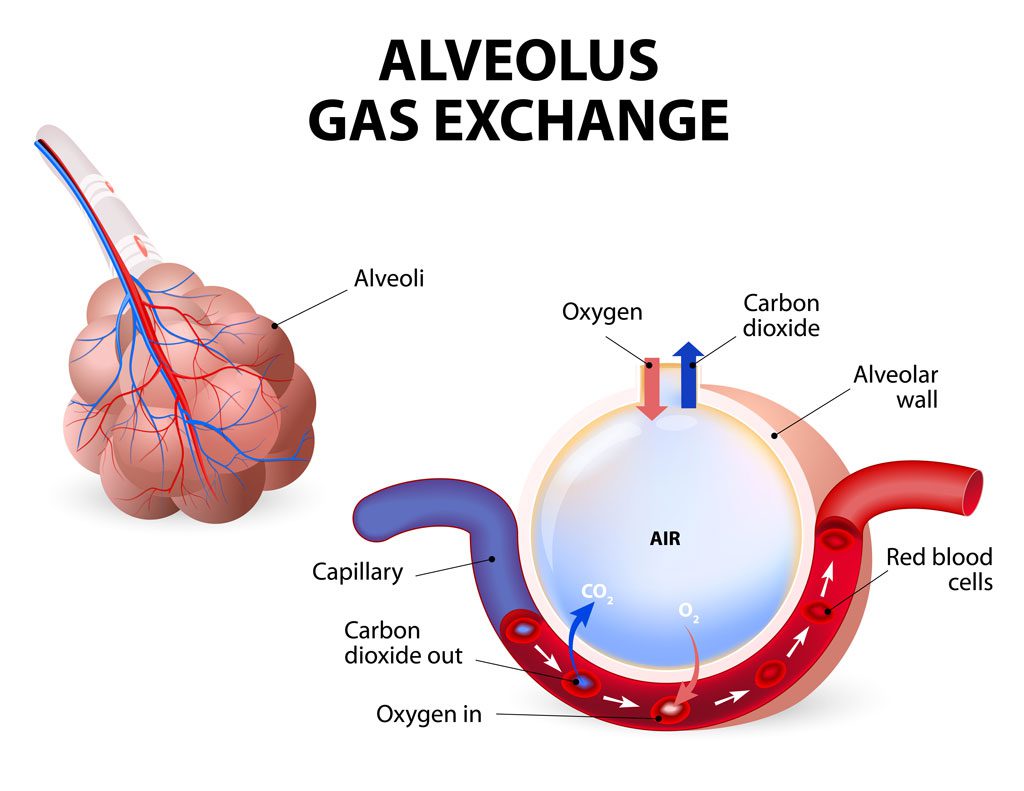
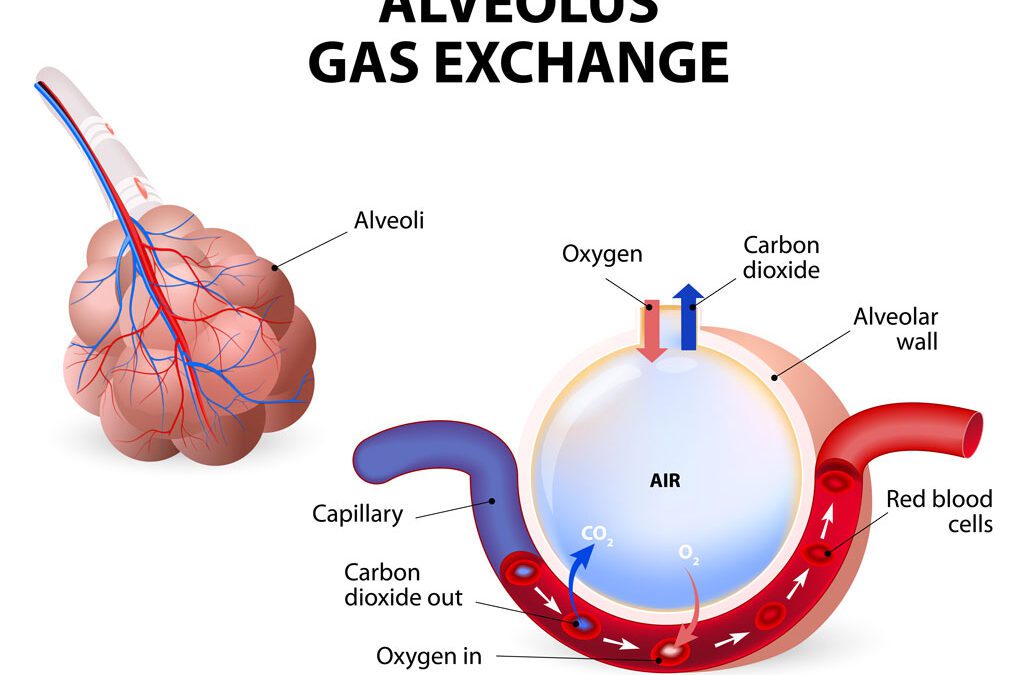
Our lungs are filled with millions of air sacs called alveolae. Added together, the surface area of all alveolar sacs is equal to nearly 70 square meters, about half the size of a tennis court. The walls of the alveoli are lined with a layer of flat cells called alveolar epithelial cells. These cells give structure to the alveoli and provide a barrier between the air and the super-thin capillary blood vessels woven between and around the alveolar air sacs. These capillaries carry deoxygenated blood pumped into the lungs from the heart.
The space between the alveolar epithelium and the blood vessels is so thin that oxygen from the air can diffuse directly through the alveolar wall and into the blood vessels. Red blood cells pick up the oxygen and are carried back to the heart to be pumped throughout the body. Likewise, waste CO2 passes from the blood into the air in the alveoli to be exhaled. This process works seamlessly every time you inhale. But infection can quickly compromise the lungs’ integrity and lead to severe disease, namely ARDS.
Defining ARDS
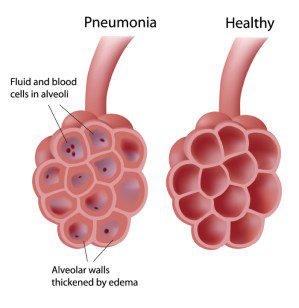
Because we are constantly breathing in pollution and bacteria, the delicate internal surfaces of our lungs are the most vulnerable tissues in the body. Luckily, immune cell monitors called macrophages patrol the alveolar epithelium and neutralize intruders. If pathogens manage to gain a foothold in the lungs these macrophages alert the rest of the immune system. This “call to war” spurns on the body’s response, called inflammation. The alveolar walls begin to swell and the capillaries beneath become porous, allowing watery fluid carrying new immune cells to flood into the alveolar space normally filled with air, leading to pneumonia. Ideally, these newly recruited immune defenders eat away any invading germs and then the process reverses itself, reabsorbing fluid and repairing the alveolar walls. But in the case of ARDS, things begin to worsen.
Inflammation can be good, as it is the body’s way of fighting infection, but out of control inflammation can become pathological. Patients suffering from ARDS have persistent lung inflammation. The thickened alveolar walls and accumulated fluid in the lungs prevent gas exchange, limiting how much oxygen the body gets with every breath. The virus SARS-CoV-2 can lead to ARDS by doing a double hit: the virus can directly kill off alveolar epithelial cells, and disrupt endothelial cells, the cells lining the capillaries surrounding alveoli, leading to more inflammation and causing a worsening cycle.
Doctors use three criteria to diagnose ARDS:
- Hypoxemia.
- An onset of within 7 days of a known insult
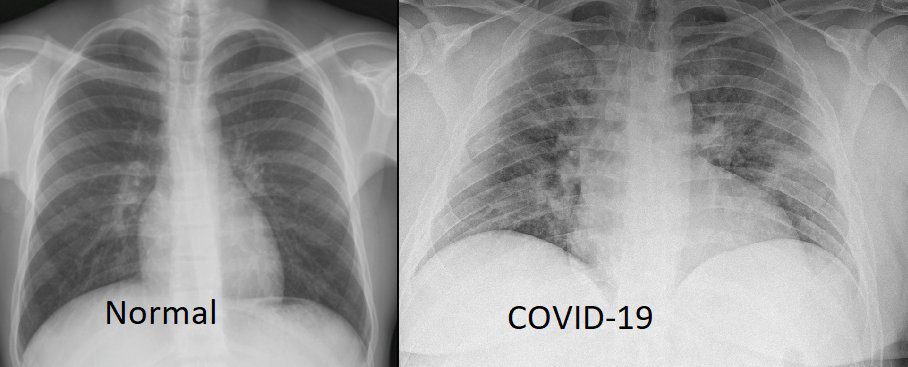
- Diffuse opacities, or dark spots, seen in x-rays or CT scans
The first hallmark of both severe COVID-19 and ARDS is hypoxemia, an inability to get enough oxygen into your system. And while the majority of severe COVID-19 patients who require breathing assistance meet the Berlin Definition for ARDS, many do not, leaving doctors to figure out why.
Complications and New Perspectives
Normally during ARDS patients experience low lung compliance, meaning their lungs can’t easily expand and contract, making their breaths raspy and shallow, worsening hypoxemia. But COVID-19 patients very often show high lung compliance, having no trouble inflating their lungs, they just can’t absorb oxygen properly. One explanation for this is that while in normal ARDS blood cannot flow properly through damaged pulmonary vasculature, in COVID-19 the blood vessels are still intact, meaning blood can still perfuse into pneumonia-filled spaces which lack any oxygen to absorb.
This significant difference from normal ARDS made early treatment difficult. In the beginning doctors emphasized the use of ventilators to help patient’s breath normally, as one would in ARDS patients. Ventilators are life-support machines which push air into the lungs, helping oxygenate the body when the patient cannot or has difficulty breathing on their own. But soon hospitals saw that putting less severe patients on ventilators wasn’t making enough of a difference in patient mortality. Physicians are now advised to have COVID-19 patients both on and off ventilators be placed in a prone position, this redistributes pulmonary blood flow into undamaged parts of the lung, significantly easing breathing and increasing blood oxygen levels.
Defining diseases using specific, research-backed, diagnostic criteria is essential for doctors to make medical decisions. Doctors are now defining a new COVID-19 specific form of ARDS called CARDS. Luciano Gattinoni, a pioneer in treating lung disease, has described two types of CARDS. The first being called the L-phenotype, characterized by high lung compliance, and the second called the H-phenotype, which is more severe and more closely resembles traditional ARDS. CARDS removes one-size-fits-all treatments and creates guidelines for ventilator settings and treatment protocols based on how the patient presents based on our growing experience with COVID-19.
The latest attempts at finding a drug capable of shortening recovery or lessening the severity of COVID-19 have pointed towards dexamethasone, a steroid drug with a long and well-studied history. Steroidal drugs work by inhibiting the immune system, meaning it may help to truncate the hyperactivated inflammatory process before it can become uncontrollable. The antiviral drug Remdesivir has also been shown to have a positive effect on survival for less severe cases of COVID-19 and could stem the infection before ARDS begins to develop. But these studies are preliminary and more work is needed to validate what is truly effective.
Helping Others Breath
So many of the standardized procedures doctors use to treat respiratory disease have been challenged by COVID-19. The effects of this disease are not something to ignore because you are not statistically at risk. Even mild cases of COVID-19 can lead to damage to the heart and lungs. The best, most effective way of reducing the risk of catching or passing on the virus is through social distancing and mask usage. Even though researchers are still trying to unravel the mechanics of COVID-19 and how best to treat it, enough is known to help stem the spread of the virus now.